
Israel could see 3rd, 4th lockdown, warns top UK epidemiologist who moved here
Michael Edelstein answers ToI’s questions, from risk of outdoor Yom Kippur prayers to herd immunity; lauds Swedish model; and cautions: ‘Real make or break comes after lockdown’
Nathan Jeffay is The Times of Israel's health and science correspondent
")
After leaving a top post in England’s COVID-19 fight and moving to Israel, epidemiologist Michael Edelstein is worriedly surveying his new country as it slides into a Yom Kippur like no other: under lockdown, in a desperate battle against the coronavirus.
Health Ministry director-general Chezy Levy warned on Sunday morning that Israel is “almost at the point of no return.” His ministry had just announced that 5,855 new coronavirus infections were confirmed Saturday, after it reported a record 8,373 new cases diagnosed on Friday.
As many Israeli Jews pray for the nation to be “sealed in the book of life,” Edelstein says its fate does indeed still hang in the balance, and will be determined by the actions of leaders and citizens.
What happens during the current lockdown is important, he said, but “the real make-or-break will come after the lockdown.”

If the country doesn’t get things right then, “there could be a third and a fourth lockdown,” he said in a wide-ranging interview on COVID-19 covering Israel’s predicament and his support for the lockdown, his admiration for the Swedish approach, and what we’ve learned about the virus so far.
Edelstein worked at Public Health England, the executive agency of the London-based Department of Health, since 2015, with responsibility for public health programs. He left the post last month to take up a professorship at Bar Ilan University’s medical school in the Galilee city of Safed, focusing heavily on “health inequalities” that affect Arab and Haredi communities.
Edelstein is also president of the infectious diseases section of the European Public Health Association and a fellow of the UK Faculty of Public Health. He has served on expert groups for the World Health Organization and the European Centre for Disease Prevention and Control, and is deputy editor of the journal Epidemiology and Infection.

Will this lockdown work?
It depends what the desired effect is. Is it possible to bring cases close to zero through lockdown? Probably not. But what it can do, in a few weeks, is to begin having an impact on the number of new cases and bring this back to a more manageable level, as well as taking hospitals out of danger of being overwhelmed.
The real make-or-break will come after the lockdown. It’s a question of whether the government will get its act together and have clear restrictions that are enforced, mass testing, and capability to trace contacts of infected people. All of this needs to be prepared when in lockdown. And it’s also a question of whether people will realize it’s serious and play by the rules. Because if not, there could be a third and a fourth lockdown. This could go on in cycles until a vaccine becomes available.

You recently arrived in Israel from the UK, and have a strong understanding of the situation in Europe and internationally. How do you assess Israel’s current predicament?
The situation in Israel is a serious situation. There’s no doubt Israel has one of the highest rates of new infection in the world and it’s a real concern. Infections and outbreaks don’t behave in a linear manner; they can be exponential. Cases went from around 2,000 a day to around 8,000 in the space of two to three weeks. That increase is very worrying, and large gatherings without adequate precautions over holidays could lead to a much bigger outbreak.
Many people are steering clear of indoor prayers for Yom Kippur, but unsure whether or not to take part in outdoor prayers. What do you think?

Evidence is that being outdoors as opposed to indoors reduces transmission, and that social distancing plus masks protects us and others. Praying in small groups outdoors and respecting the two-meters rule can reduce risk, though there are things to consider, such as whether really loud singing may be an issue that increases risk. The same goes for when a small service becomes much larger if people start bringing families and kids, and the size of the gathering grows. If conducted responsibly, I think the risk of outdoor prayer is low.
How did we get to the current situation, from the success story of the first wave to the first country back in lockdown?

The mistake Israel made first time around was, after the first lockdown, giving people a sense that it was over and we can go back to normal and don’t need to worry anymore. Coronavirus is not going to go away anytime soon, but we know from some examples, like Sweden, that if there are successful measures in place it’s possible to keep it at a manageable rate.
The purpose of lockdown is not to get back to normal but to get a situation in which we can reopen. But it’ll be in a controlled way with restrictions. It’s possible to live this way consistently for a long time. If people make the same mistake again and think we can go back to normal, we’ll be in third lockdown. But it’s hard to convince Israelis.
We’ll return to Israel’s situation in a moment, and also find out more on your thoughts about the Swedish approach. But first, let’s talk briefly about the virus itself, which is still baffling doctors. We’ve had more than half a year to become familiar with it. What are the most important things we know now that we didn’t know in March?
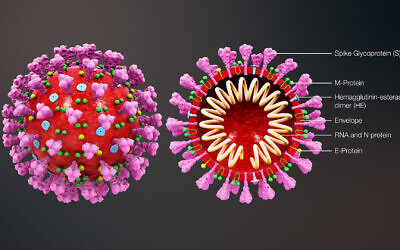
Some factors that affect risk levels are very well understood now. Age is an important factor. Having chronic health conditions, especially respiratory, is an important factor, but none of this explains why some people who are young become very sick and some people who are older don’t. What we understand more and more is how the virus attacks body and binds to ACE2 receptors — which are like docking stations that sit on the outside of the cell, and the virus attaches there — and research suggests people have different forms of the receptor that make the body more susceptible to the disease, while others are less susceptible.
Young children don’t get infected that easily and aren’t a major driver for the virus, unlike with flu. And one hypothesis is they don’t have a developed form of this receptor. Ethnic factors are relevant and it seems there is a combination of genetic makeup and social and economic factors.

Is there anything people can do, beyond hygiene measures and social distancing, to protect themselves?
One of the factors that affects whether you get very ill if infected is the status of your body, and in this context obesity is a big factor. If you have a balanced diet and exercise regularly, you have better chances. The idea that vitamin D offers a benefit is an interesting theory, but it is still unclear.
The pandemic is very confusing for people, as many still don’t fully understand what symptoms they should be looking out for. What is your latest assessment?
One of the challenges of COVID-19 is that most of its symptoms are shared with other diseases such as flu or even the common cold. The most widespread symptoms are cough and fever. If you get cough or fever there’s no way of knowing from symptoms whether it’s COVID-19 or something else. The threshold for being tested should be really low. The slightest symptoms should trigger testing. There’s a fear of being quarantined following testing. But failure to get tested puts loved ones and strangers at risk. There are other symptoms like badly losing your sense of smell and sense of taste. So people with systems including fever, cough, difficulty breathing, and loss of taste or smell, should get tested.

(RyanKing999/iStock by Getty Images)
What is your snapshot explanation of the causes for spiraling case numbers in Israel?
It’s a combination of factors. There was, until recent, some unclarity about who leads coronavirus response. The other thing is there’s clearly a behavioral component and there’s quite a lot of complacency in Israeli society, with people holding large gatherings and sometimes not wearing masks. There are people with symptoms who don’t get tested, which has an impact, and there are cases of people not getting tested because they don’t want to be quarantined. There are also lots of people living in crowded neighborhoods and multi-generational households. It’s not about blaming people but about understanding different factors.
Are high infection rates among Arabs and Haredim due to circumstances faced by the communities, or their conduct?
It’s not a black-or-white situation, but a combination of both.
Tell us more about your thoughts on the approach of Sweden, which assiduously avoided lockdown.
Having a complete lockdown for very extended periods of time is very hard to assert. It’s hard, and people lose income and ability to live. Sweden didn’t have a lockdown. It was heavily criticized but there’s a balance. Sweden made a deliberate choice to have more cases, but to allow life and the economy to continue functioning. In Israel we put a very high value on individual lives. It reflects Jewish ideals in many ways, and this informed early responses. Personally, I believe in balanced approaches and I think Sweden made a bold move at a time when there was very little evidence, but retrospectively, it was a sensible thing to do, particularly if you can protect people who are very vulnerable.
I think the way Sweden did things is, in a sense, what Israel was doing now in practice until the second lockdown. It’s wasn’t an explicit policy but this approach enables a degree of infection and keeps almost everything open. We know there’s a price to pay for keeping society open. However, if people are not sensible, ignore the recommendations and don’t get tested, we will see a rapid increase in the number of cases that could mean higher deaths and overwhelmed hospitals. We’re learning that we can manage without full lockdown, but it only works if people play by the rules.

Some people may think you are contradicting yourself, saying it’s right that we’re in lockdown, but on the other hand can learn from the Swedes. Can you clarify?
It’s not a contradiction. It really depends at what point you are in the epidemic. Any country, at Israel’s current level of transmission, needs a lockdown. If Sweden had this level of transmission, it would also go to lockdown. But if there were steps that had been taken after the first lockdown, [the Swedish model] would have worked. In Sweden there were low-level restrictions and people stuck to them. It really depends on timing, public willingness to hold by restrictions, and public trust. In Israel, trust in government is low, while in Sweden it’s high.
We are hearing some suggestions that Israel is nearing herd immunity. The assumption is that many more people have been infected than test numbers show, and the threshold for herd immunity is lower than imagined. What do you say?
Israel is nowhere near heard immunity, even after accounting for under-diagnosis. It is not clear what percentage needs to be infected to achieve it but it’s impossible to achieve that with a modest percentage.
You were heavily involved in the response in England before coming to Israel. How do the two countries compare in terms of the coronavirus?
In a sense the English and the Israeli experience are almost polar opposites. At the very beginning, England was one of the later countries to impose restrictions and a lockdown, and this led to high levels of transmission and a high number of cases early on. Though the numbers looked bad at the time, this led to a significant part of the English population being infected early on, including the most vulnerable such as nursing home residents. So this meant there were less people to infect two to three months later, especially among vulnerable groups. This meant there’s less of a pool of people to be infected in the second wave.
Israel had very strict regulations early on and as a result of that had fewer infections and fewer deaths. But in a sense there’s a price to pay for that — as people who are vulnerable weren’t infected early, and got infected when the restrictions were relaxed.

Are there any common features to the two countries?
One thing neither country has done particularly well is find the right balance between allowing people to carry on with their lives while minimizing the risk of infection. This requires, among other things, tracing all contacts of each case. Contact tracing hasn’t been done optimally in either country, but if you’re able to do it, you can have more freedom of movement.
England’s Jewish community has been particularly badly hit by coronavirus deaths. Is there any explanation?
The Jewish community in England has a uniqueness. The first aspect is the Jewish community is much older than the general population. Also, Purim coincided with start of outbreak, when awareness wasn’t high, and Purim parties were a real catalyst for this.

Can you explain the latest thinking, as you understand it, on how the virus spreads? At first, there was lots of emphasis on the danger of picking up the virus from surfaces, and hand hygiene, while now the talk is more about droplets, and there is some talk of the virus being aerosolized, meaning turned into small droplets that may be able to hang around in the air.
The virus lives in the respiratory system and when someone coughs, their infected droplets travel. It can survive a certain amount of time on surfaces. Early on, there was much more emphasis on surfaces, now it’s more emphasis on person-to-person droplets. It’s quite a big virus in terms of size, so it doesn’t travel that far. There are studies suggesting it can be aerosolized, but it is unclear how much of a role that plays and the main method of transmission is droplets going from person to person. The idea it can float into air is unlikely to be a major mode of transmission. In viruses you see that are commonly aerosolized, there are higher rates of transmission.


 and Prime Minister Benjamin Netanyahu walk into Trump's Mar-a-Lago club, December 29, 2025, in Palm Beach, Florida. (AP/Alex Brandon)")
; Opposition Leader Yair Lapid leads a Yesh Atid faction meeting at the Knesset in Jerusalem, June 15, 2026. (Yonatan Sindel/Flash90); Gadi Eisenkot, head of the Yashar party, speaks during a conference at Tel Aviv University, May 12, 2026. (Avshalom Sassoni/ Flash90); Minister of Finance Bezalel Smotrich holds a press conference ahead of the vote on the state budget at the Knesset, June 15, 2026. (Yonatan Sindel/Flash90)")
")
; A woman holds up an Iranian flag in front of a banner showing a portrait of the Supreme Leader Ayatollah Mojtaba Khamenei, in Tehran, June 4, 2026. (AP Photo/Vahid Salemi); US President Donald Trump attends the UFC Freedom 250 on the South Lawn of the White House, June 14, 2026. (AP/Alex Brandon)")
")
")
")
")
The Times of Israel Community.